Findings of Homecare Association member survey, April 2022
Summary
Demand for homecare is outstripping supply. Councils are reporting high levels of unmet need in the community and NHS hospitals are struggling to discharge people back home. Inadequate capacity in homecare and other community services is contributing to greater burdens on the NHS, including more people with deteriorating health; longer ambulance waits; inability to respond fast to all emergencies; cancelled clinics; cancelled operations; and difficulty in reducing waiting lists.
Though 16% more hours of homecare have been delivered over the last year, retention and recruitment of homecare workers is harder than ever. Many factors, both long- and short-term, influence retention and recruitment of homecare workers and thus workforce capacity.
On top of underlying poor pay, terms and conditions of employment, which stem from inadequate government investment in state-funded homecare, the sector has also been adversely affected by Brexit, COVID-19 and now international conflict. Tightening of labour markets, pressure on supply chains and rising energy costs are fuelling inflation. This is leading to a rapid rise in business costs and cost of living, placing further pressure on low-paid workers and their employers. Unlike other business sectors, where increased costs can be passed to consumers, state-funded homecare agencies are unable to charge councils high enough fees to cover rising costs, as the latter have limited budgets and monopsony purchasing power. Some local authority fee rates for homecare do not even enable compliance with the legal minimum wage, never mind cover escalating operational costs, such as wages, sick pay and fuel.
To make matters worse, many homecare workers are now not being paid or are receiving low pay whilst being required to isolate after a positive COVID-19 test result, following removal of the Infection Control and Testing Fund (ICTF) by the government on 31 March 2022. Though COVID-19 restrictions have been lifted for wider society, they remain in place in health and social care due to the higher risk categories of people drawing on services. Almost half of homecare workers are on zero-hour contracts due to zero-hour purchase of homecare by councils, so they are paid only for hours worked.
To investigate the impact of removal of the Infection Control and Testing Fund on the homecare workforce and, in turn, on people needing and receiving care, we conducted a survey of Homecare Association members during April 2022, representing just over 31,350 careworkers supporting nearly 46,200 older and disabled people.
Key findings were as follows:
- Among those in receipt of the third and final round of the Infection Control and Testing Fund, 85% of respondents either paid full wages to staff who were self-isolating due to COVID-19 throughout the six months or did so until there was no more grant money available. Only 7% were paying Statutory Sick Pay rather than full pay.
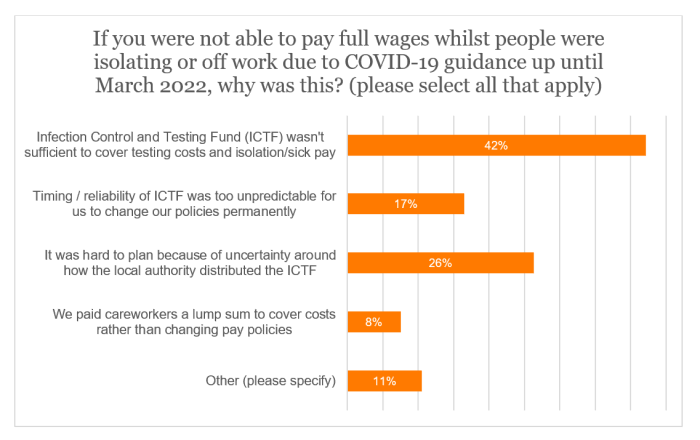
- When applicable respondents were asked to select all options as to why they were unable to offer full wages (either throughout or at any point) for those self-isolating or not working due to COVID-19 up until March 2022, 42% concluded that the ICTF had not been adequate to cover costs (of those that selected this answer and stated their funding source, half were predominantly in the self-funding market, where allocation of the ICTF was patchy). Meanwhile, just above a quarter (26%) were stymied by uncertainty on ICTF distribution.
- Now the ICTF has ceased, only 6% of providers claimed that they typically offer full sick pay. Using the figures provided by respondents, this means that an estimated 96% of careworkers are receiving no pay or low pay whilst isolating after a positive COVID-19 test.
- Close to half (48%) asserted that careworkers were seeking alternative employment due to issues regarding loss of pay while isolating. Almost a fifth (18%) stated that careworkers had indeed resigned for this reason.
- 59% of the sample expressed anxiety that staff will come to work after testing positive for COVID-19. The same proportion (to the nearest whole number) noted the added difficulty in recruitment due to staff not being able to provide care after a positive test and then not receiving full pay.
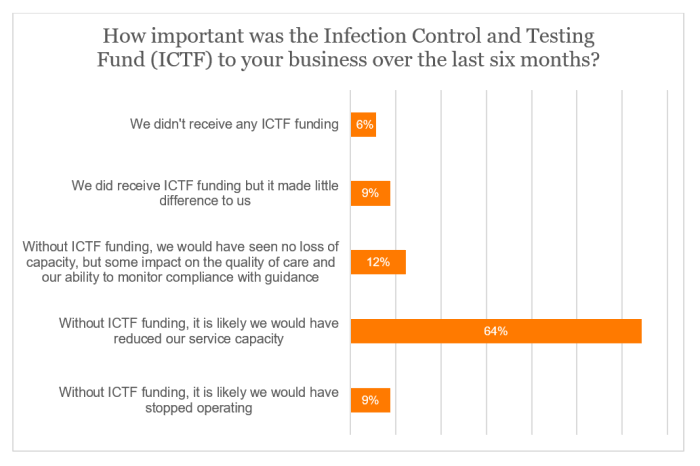
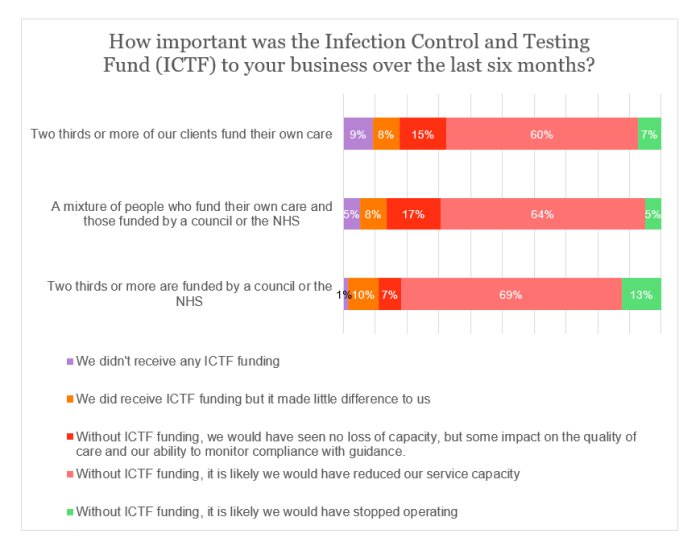
- Approaching two-thirds (64%) of the sample elucidated that their service capacity would have probably been reduced without the ICTF. An additional 9% claimed that their business would have likely closed without the funding. On this metric, there was a clear distinction between the state-funded and self-funded parts of the sector. While a combined 82% of those reliant on council or NHS funding would have likely reduced capacity or stopped operating without ICTF funding, the same could be said for only 68% of those in the private-pay market.
- In excess of three-fifths (61%) of the sample asserted that, as a result of staff sickness or isolation, existing clients were still being supported, but new referrals were being declined. Moreover, 11% claimed that they were also handing work back and ending support for some existing clients.
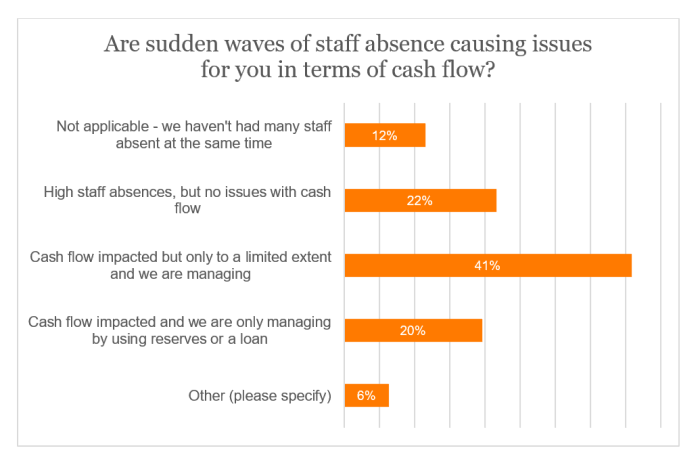
- 41% of respondents claimed that, due to sudden waves of staff absence (up to 30% in some cases, though more typically up to 10%), their cash flow had been affected, but they have still been able to cope. More worryingly, a fifth were now reliant on using their reserves or a loan.
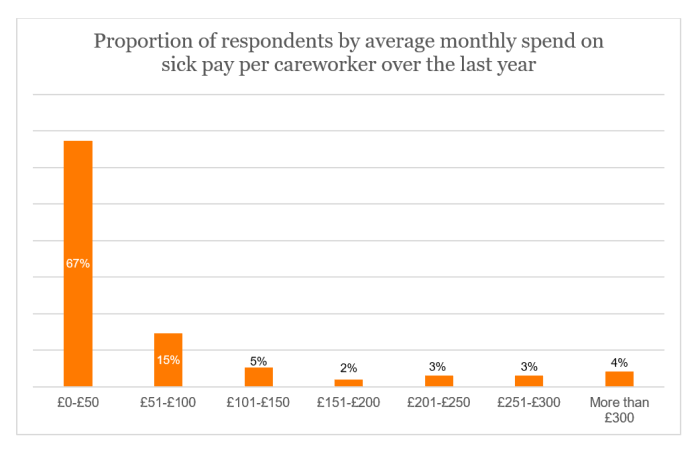
- Across all respondents, the estimated average monthly spend on sick pay was £47 per careworker during the last year. 11% had an average spend of more than £200 per careworker.
Conclusion and recommendations
The Infection Control and Testing Fund, whilst unpredictable and time-consuming to administer, was invaluable in terms of maintaining workforce capacity and morale during COVID-19. Many services would not have remained viable without emergency funding from the government, for which the homecare sector is extremely grateful.
It needs to be remembered that whilst COVID-19 restrictions have been lifted in wider society, testing and isolation is still required in the health and care sectors, including homecare.
Councils pay homecare providers in arrears for client contact time only. Thus, providers do not receive sufficient income to cover two sets of wages for one call, if one careworker is covering while another is isolating. In the absence of emergency COVID-19 funding, therefore, most homecare workers are not being paid at all until day 4, when Statutory Sick Pay of £99.35 per week can be claimed, itself at least a 2 to 3-fold reduction over normal wages. Many people continue to test positive for 10-11 days.
At a time of rapidly increasing cost of living, especially fuel costs which we have previously reported to be a particular issue for homecare, it is hardly surprising that retention and recruitment of careworkers is being badly affected by loss of pay.
Ultimately, older and disabled people who need homecare services are suffering the consequences of underfunding and inadequate workforce capacity and remain unable to access the care they need. This risks deterioration in their health, reducing their wellbeing and adding to pressure on more expensive services. Delayed discharges from hospital, affected by lack of capacity in homecare and other community services, also make it difficult for the NHS to respond in a timely way to emergencies and to reduce waiting lists. Regrettably, some people are dying before their time due to insufficient investment in social care and health services by central and local government.
We continue to urge the government to:
- Reinstate emergency COVID-19 funding for social care to enable careworkers to receive full sick pay whilst isolating;
- Pay for a temporary fuel allowance to cover the increased costs of fuel for vehicles needed to deliver homecare; and
- Invest properly in homecare so we can build capacity and reduce unmet need, recognising that NHS hospitals will never succeed in reducing their waiting lists if they cannot free up beds by discharging people back home.
Introduction
Demand for homecare is outstripping supply. Councils are reporting high levels of unmet need in the community, and the latest survey from the Association of Directors of Adult Social Services (ADASS) shows that over half a million people are waiting for assessment and care. NHS hospitals are struggling to discharge people back home due to inadequate capacity in homecare and other community services. Prolonged stays in hospital when people are ready to go home increase the risk of infection and deterioration in physical and mental health. Delayed discharges also mean that hospital beds are unavailable for new admissions, which contributes to increased ambulance waits, cancelled clinics and cancelled operations. This makes it difficult for the NHS to respond in a timely way to emergencies and to reduce waiting lists. Regrettably, some people are dying before their time due to insufficient investment in social care and health services by central and local government.
Homecare hours delivered have increased by 16% over the last year but, despite this, ADASS reported a 7-fold increase in commissioned homecare hours left undelivered, as there are not enough homecare workers. Indeed, the vacancy rate in homecare is increasing and, in April 2022, reached an all-time high of 13.5%.
Many factors, both long- and short-term, influence retention and recruitment in homecare and thus workforce capacity.
Poor pay, terms and conditions of employment have long been a problem for the workforce, particularly in the state-funded part of the sector which represents 70% of the whole. These stem from inadequate funding by central government and poor practices in commissioning and purchase of homecare by public sector organisations.
In recent years, the homecare sector has also been adversely affected by Brexit, COVID-19 and now international conflict. Tightening of labour markets, pressure on supply chains and rising energy costs are fuelling inflation. This is leading to a rapid rise in cost of living, which is placing further pressure on low-paid workers and their employers.
Fuel costs have increased by 30-37% over the last year and homecare workers, who collectively drive an estimated 4 million miles per day, are struggling to fill their tanks. Our research indicates that many homecare workers receive only 10p per mile, whilst NHS staff receive 54p per mile. In a recent survey of homecare providers, half of respondents asserted that careworkers had requested an increase in the mileage rate, while more than a fifth (21%) added that careworkers had either given notice, intended to look for work elsewhere or had already done so because they cannot afford to put fuel in their cars.
Many homecare providers serving the state-funded part of the sector are operating with slim margins and are unable to charge councils high enough fees to cover costs, as the latter have limited budgets and monopsony purchasing power. Some local authority fee rates for homecare do not even enable compliance with the legal minimum wage, never mind cover escalating operational costs.
To make matters worse, many homecare workers are not being paid or are receiving low pay whilst being required to isolate after a positive COVID-19 test result, following removal of the Infection Control and Testing Fund (ICTF) by the government on 31 March 2022.
Unlike wider society, isolation after a positive COVID-19 test is, rightly, required by government guidance for the health and care sectors. For the first three days of absence, many homecare workers on zero-hour contracts (almost half of the total) receive no pay at all, and from day 4 onwards, they receive only Statutory Sick Pay (SSP) of £99.35 per week, which is 2-3 times lower than the average weekly wage at the national legal minimum. It is common for people to test positive for at least 10-11 days. The resulting loss of income is having a further negative impact on retention and recruitment of homecare workers. This follows an estimated loss of 18,000 to 40,000 homecare workers who left the sector after the consultation was announced on requiring vaccination as a condition of deployment, though they withdrew the proposal at the eleventh hour following evidence-based campaigning.
To investigate the impact of removal of the Infection Control and Testing Fund on the homecare workforce and, in turn, on people needing and receiving care, we conducted a survey of Homecare Association members. Details of the survey method and results obtained are given below.
About the collection method and response rate
Responses were collected through a self-selecting online survey of Homecare Association member organisations between 11 and 26 April 2022. Responses were received and accepted from 292 homecare providers, large and small, state-funded and private-pay funded, across England (with two responses also received from providers in Wales). This represented just over 31,350 careworkers supporting nearly 46,200 people in their own homes.
In our analysis of answers, we have excluded the very small number of responses stating that they did not know (or preferred not to say) the answer to one or more individual questions, as well as responses that were not relevant to the question (when required).
Organisations completing the survey
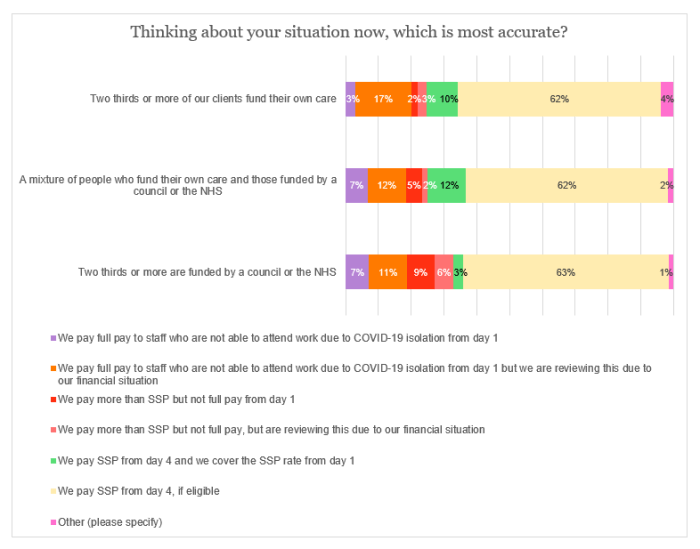
The survey was completed by providers serving either predominantly state-funding or self-funding clients, or a mixture of both, as illustrated by the graph below.
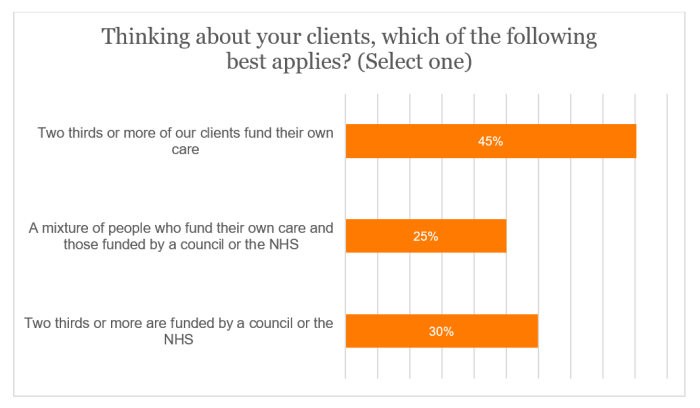
NB. Data labels on the graphs have been typically rounded to the nearest whole number. Where percentages have been, for example, added or subtracted, exact figures have been used – hence, there may be occasional rounding differences from the graph labels.
Results
Infection Control and Testing Fund (ICTF)
Approaching two-thirds (64%) of the sample elucidated that their service capacity would have probably been reduced without the ICTF. An additional 9% claimed that their business would have likely closed without the funding.
On this metric, there was a clear distinction between the state-funded and self-funded parts of the sector. While a combined 82% of those reliant on council or NHS funding would have likely reduced capacity or stopped operating without ICTF funding, the same could be said for only 68% of those in the private-pay market.
Among those in receipt of the third and final round of the Infection Control and Testing Fund, 85% of respondents either paid full wages to staff who were self-isolating due to COVID-19 throughout the six months or did so until there was no more grant money available. Only 7% were paying Statutory Sick Pay.
One comment postulated among those replying ‘Other’ was:
“We received very little financial support from the local authority's Infection Control and Testing Fund as we were not a preferred provider for the council. Therefore, the grant we received did not cover costs for isolation. We topped up for people initially – however, we were not able to continue to do this, as this would have affected the cash flow of the business and would have meant using money from the business.”
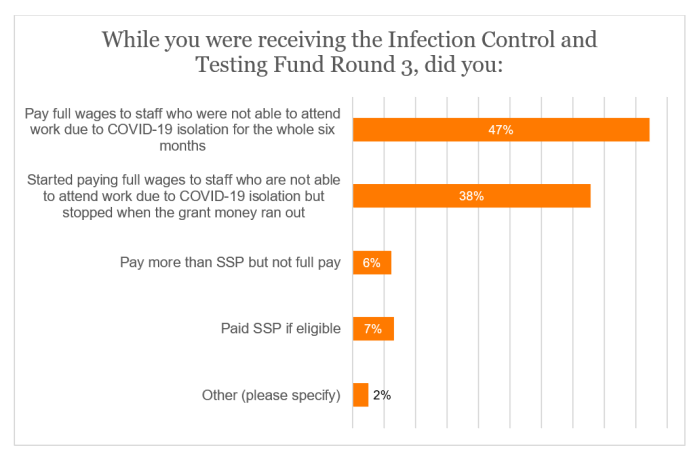
When applicable respondents were asked to select all options as to why they were unable to offer full wages (either throughout or at any point) for those self-isolating or not working due to COVID-19 up until March 2022, 42% concluded that the ICTF had not been adequate to cover costs (of those that selected this answer and stated their funding source, half were predominantly in the self-funding market). Meanwhile, just above a quarter (26%) were stymied by uncertainty on ICTF distribution. Within the ‘Other’ category, comments typically focused on the ability to offer full pay while ICTF was available.
Inability to pay full sick pay
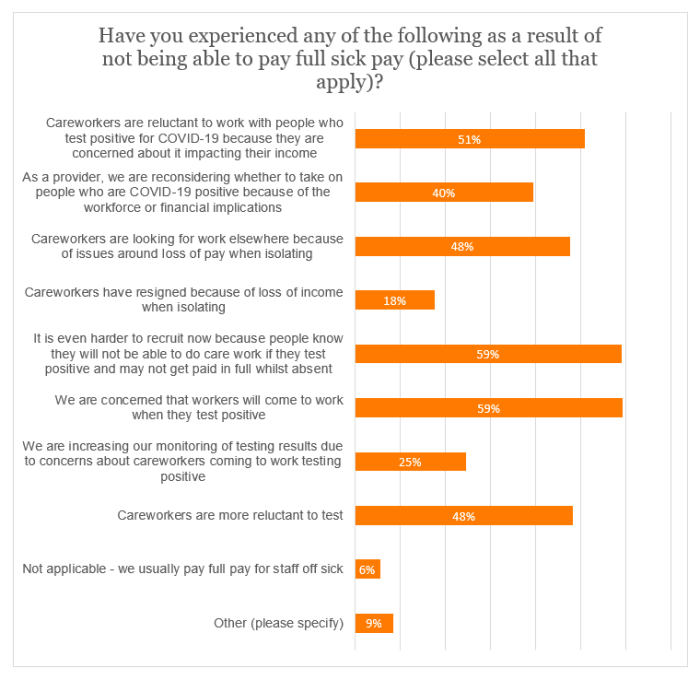
Respondents were presented with a range of options to demonstrate the effect of not being able to offer full sick pay and asked to select all that apply.
Close to half (48%) asserted that careworkers were seeking alternative employment due to issues regarding loss of pay while isolating. Almost a fifth (18%) stated that careworkers had indeed resigned for this reason.
59% of the sample expressed anxiety that staff will come to work after testing positive for COVID-19. The same proportion (to the nearest whole number) noted the added difficulty in recruitment due to staff not being able to provide care after a positive test and then not receiving full pay.
Only 6% of providers claimed that they typically offer full sick pay. Using the figures provided by respondents, this means that an estimated 96% of careworkers are receiving no pay or low pay whilst isolating after a positive COVID-19 test.
Within the ‘Other’ option, a few respondents were concerned that they would no longer be able to offer full sick pay due to the loss of government funding. Here are some of the more salient comments:
“If the Infection Control [and Testing] Fund is not continued, I would feel it is my responsibility and duty to our staff to inform them about the Care Workers' Charity and to apply [for support] if they are eligible. This will result in a significant increase in the number of applications. If staff are going to lose income by isolating, they will be forced to turn to other sources of income. They may have increased reliance on charity or foodbanks, and some may fall into debt. Faced with these choices, it is highly likely that some will leave to work in other sectors where isolation is not compulsory.”
“SSP [Statutory Sick Pay] really is not working, as they have to be off for 3 days before getting anything. Some of our carers work a 40-hour week and only earn the sum of a couple of hours a day on sick pay.”
“Care workers are asking for holiday so that they have some income whilst they are required to isolate as they cannot afford the loss of income.”
Staff absence rates
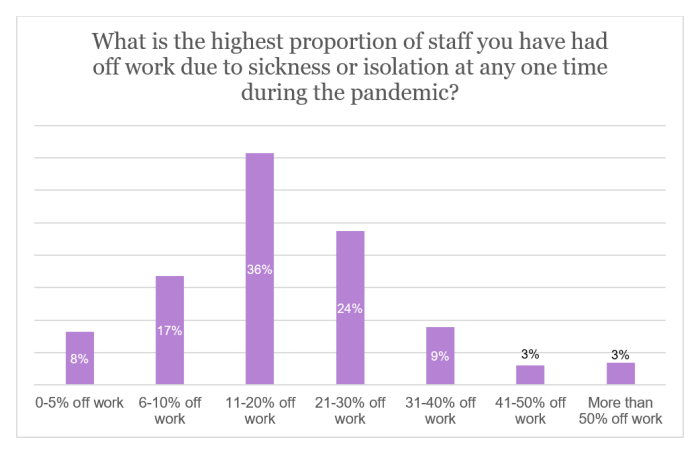
As it stands, more than two-thirds (68%) of respondents have up to (or equal to) 10% of their staff off work because of sickness or isolation. Only a small proportion of the sample (3%) have a current absence rate of more than 30%.
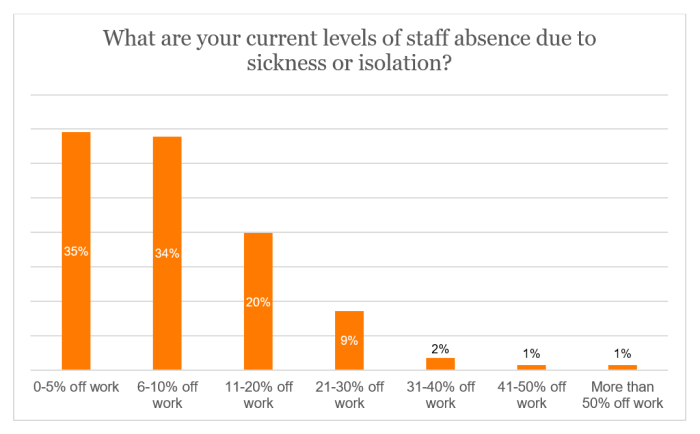
In contrast, nearly three-fifths (59%) of providers asserted that their highest absence rate during the COVID-19 pandemic was between 11% and 30%. A further 15% witnessed over 30% of their staff being absent at one point.
The sample was asked if they had any additional comments on staff absence levels. Alarmingly, some respondents postulated that the situation is now worse than at any time during the pandemic. A handful of respondents also made mention of related issues, such as long COVID or staff burnout. Two providers alluded to staff being off work for 11 days, due to the requirement for two consecutive negative lateral flow tests before they return to work.
Among the comments were the following:
“It is not just the number of staff off, but the fact that testing just before the shift means you cannot plan cover in advance. Often, services find that several staff members test positive at the start of the shift, and they are then scrabbling around to try to provide adequate care… Our managers have said they live in constant fear of the test results...This is also contributing to burnout and an increase in stress-related sickness.”
“We, like others in the sector, are concerned that without the ability to pay full sick pay, staff will not register positive test results and may choose to leave the sector for industries where they can work if well enough to do so following a positive test.”
“Staff isolating due to COVID has put more pressure on those able to work, which has then increased their sickness levels.”
“Staff absence is a constant worry [and] not just COVID-related… Because of absence, people get fed up pulling in extra hours, with little extra remuneration due to existing profit margins. We are unable to offer better incentives to prevent absence.”
“Staff with young children have to also stay at home… if they cannot attend school due to COVID... [A] high percentage of carers are single mothers, so this also has an effect on staff unable to work.”
Effect of staff absence rates
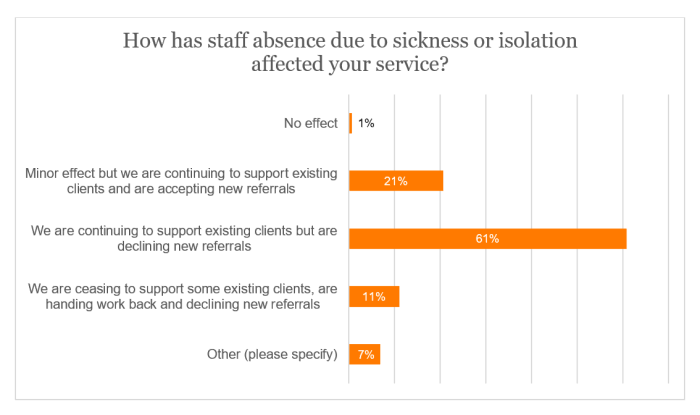
In excess of three-fifths (61%) of the sample asserted that, as a result of staff sickness or isolation, existing clients were still being supported, but new referrals were being declined. Moreover, 11% claimed that they were also handing work back and ending support for some existing clients. Within the ‘Other’ category, comments included:
“We are only able to take on new customers when another customer leaves. We are sometimes having to reduce call times or ask [the] family to assist as we cannot cover all calls due to staff absences.”
“We have had to use [the] office team to cover visits, and we have limited ability to accept new clients and are operating a waiting list.”
“We have had to reduce the business size by a ¼. [The] business is making a loss financially and we are just trying to get by.”
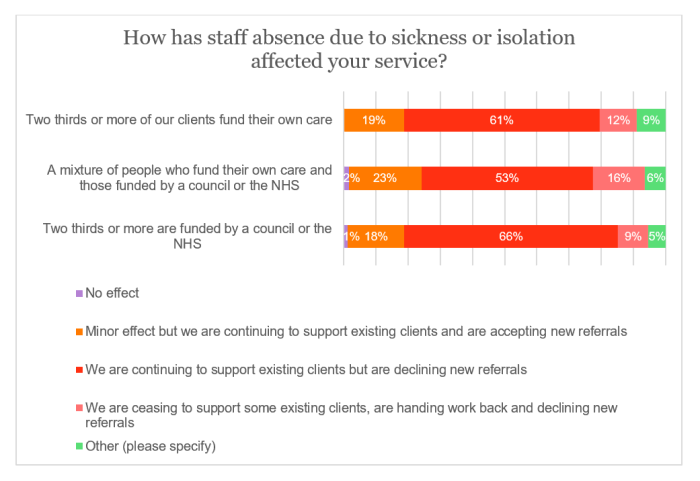
When breaking the data down by funding source, we see that around two-thirds (66%) of those respondents that are predominantly state-funded are declining new referrals while still supporting current clients, compared with 53% for those whose funding is a mixture between state and self-funders. Interestingly however, this narrative is reversed in the case of support for some existing clients being ceased and work handed back (as well as new referrals being turned down), with the proportion for mixed-funded providers being seven percentage points higher than that for those who are state-funded.
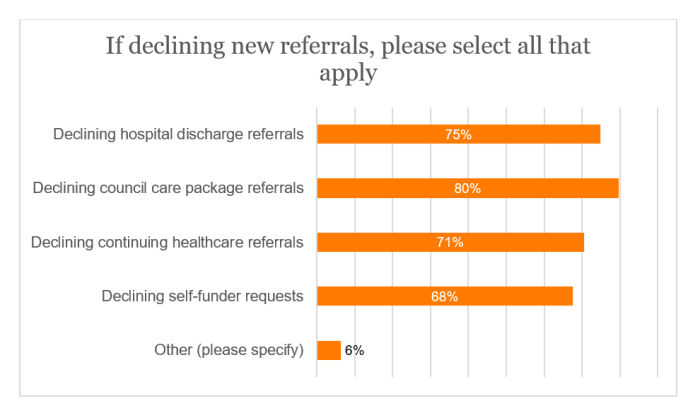
Among respondents who are declining new client referrals, four-fifths were rejecting council packages, while three-quarters were turning down hospital discharge referrals (Note that the sample was asked to select all options that applied).
For those that selected the ‘Other’ category, the comments included:
“We only take new customers to replace customers that leave, only self-funding.”
“Taking occasional very small packages if another client passes away.”
“Assessing on a day-to-day basis and declining where required.”
Cash flow issues
41% of respondents claimed that, due to sudden waves of staff absence, their cash flow had been affected, but they have still been able to cope. More worryingly, a fifth were now reliant on using their reserves or a loan.
Three of the most noteworthy comments made in the ‘Other’ category were as follows:
“So far, we have managed to cover virtually all visits... However, to achieve this, I have the entire office team out doing care calls (including the owner) and am asking already tired and frazzled other members of staff to do many more hours than they are usually happy to provide. The fatigue across our entire team after the first 2 years of Covid has been huge, but in the last 6 months, the stresses have very obviously increased significantly. This whole issue is a broader one about morale in the workforce, and the likelihood that it will accelerate people simply deciding they have had enough and leaving the sector. Not just caregivers, but care managers (I am aware of a big increase in the attrition of Registered Care Managers in the sector) and owners (in our case, the owner [has] barely [taken] home a salary himself for 3-4 years now, in an effort to ensure his staff are looked after). This is not sustainable.”
“We cannot sit back and not support the staff who are isolating. We are juggling finances around to ensure we top up their wages for this period, but this is not sustainable moving forward. We are using reserves to do this, but the government has to support the sector, otherwise it will be financially not sustainable, staff will leave, or we will not be a financial position to continue.”
“We are very worried about how we will survive whilst paying people to be off sick (some managers paid full pay) and paying full pay for carers to cover. We cannot take on new service users as we are terrified [that] staff will be isolating and we won’t be able to cover.”
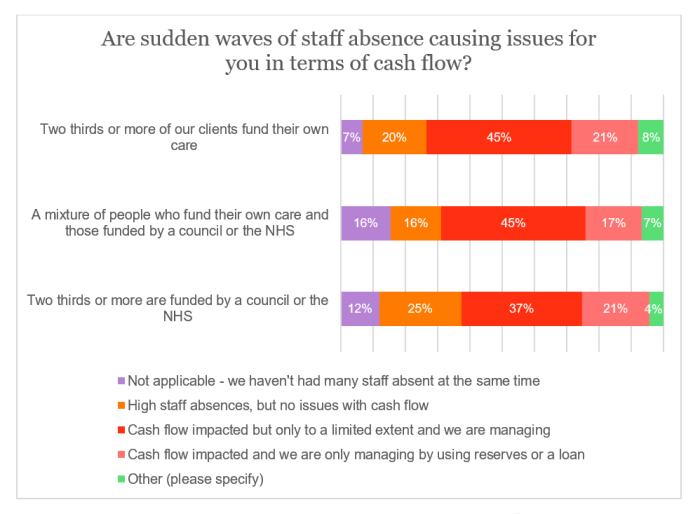
A fifth of those predominantly in the self-funding market concluded that they had no issues with cash flow despite high staff absences, compared with a quarter of those who are state funded. However, the respective proportions for those managing only by using reserves or a loan were the same (21% to the nearest whole number).
Spend on sick pay
The sample was asked for the average monthly spend on sick pay for all careworkers in their organisation over the last year. By dividing the respective figure by the number of careworkers, this will give us the average per careworker for each organisation (with both sets of data being cleaned before analysis).
Across all respondents, the estimated average monthly spend on sick pay was £47 per careworker during the last year. Indeed, as shown in the graph below, the average outlay for around two-thirds (67%) of providers was between £0 and £50 per careworker. 11% had an average spend of more than £200 per careworker.
Current sick pay offer
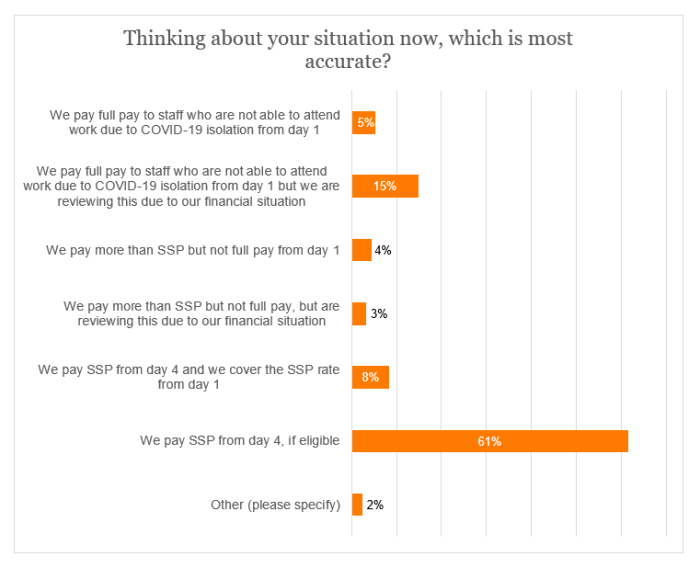
With the Infection Control and Testing Fund now withdrawn, over three-fifths (61%) of the sample are now only paying Statutory Sick Pay (SSP) from day 4, if eligible, with a further 8% doing this but covering the SSP rate from day 1.
When combining these figures and comparing with before, only 6% of respondents currently paying SSP were also doing so during ICTF Round 3 (if they received funding); indeed, 87% of this subset were paying full wages either throughout or until funding ran out.
When splitting the data according to funding source, a similar situation is seen across the board. Yet, the proportion of mainly self-funding respondents paying SSP now (either from day 4 or covering the rate from day 1) is six percentage points higher than those in the state sector. The same points difference (to the nearest whole number) is apparent between private-pay and state-funded providers on full pay being paid, but this is being reviewed for financial reasons.
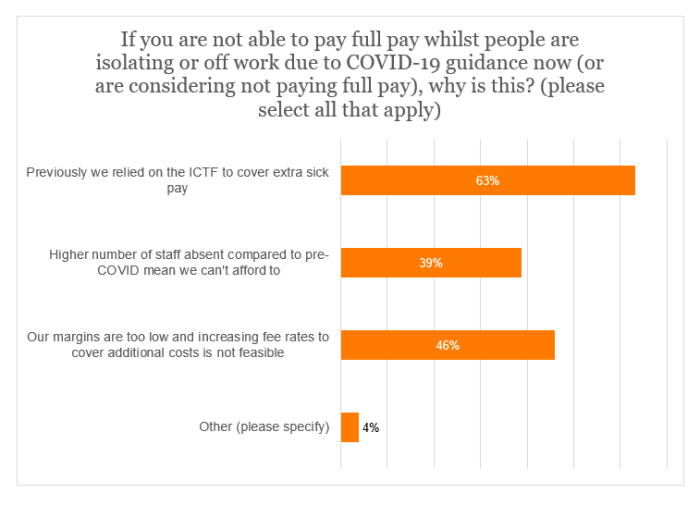
For those currently unable to offer full pay or those that are doing so but are now reviewing the situation, approaching two-thirds (63%) of the applicable sample said that they had been reliant on the ICTF in order to cover this. In addition, 46% asserted that this was not possible due to low margins (with respondents asked to select all that apply).
One commenter in the ‘Other’ category mentioned that, as well as COVID-19, there was “so much absence due to mental health issues.”
Further comments
Respondents were asked if they had any additional comments about sick pay or the Infection Control and Testing Fund. Many of the comments followed a similar theme, as illustrated by the following:
“Sick pay is the biggest threat to the financial viability of the sector at present, and unless addressed, will result in many businesses collapsing.”
“[I] think it makes no sense to remove the funding and yet still require staff to continue to isolate in line with requirements. It feels disingenuous by the government - our margins are so tight already that we cannot afford to pay for COVID isolation.”
“We really need the funding just to pay carers when isolating. They cannot afford to lose wages and we cannot afford to pay them full wages. We are and will continue to lose carers.”
“SSP should always be from day one and the amount needs to be higher – rent and bills are not reduced if you are sick; one's costs remain the same. Patients are being put at risk because not everyone can afford to take time off – this also affects their wellbeing and makes them… more susceptible to more sickness as they are then run down.”
“[The] NHS pay their staff in full and yet we are not funded to do the same, even though we have to work with the same guidance. Just like testing, it is an example of harsher terms for private companies than the NHS.”
“This fund has been invaluable in terms of maintaining staff morale during an exceptionally difficult period... Our service would not be financially viable without the Infection Control and Testing Fund, given all the additional overheads we have had to bear during the COVID period. It needs to be remembered that this period has not ended, given the need to continue to test and self-isolate and we would therefore strongly recommend that some government support is reintroduced.”