Why vaccination against COVID-19 is a good idea and regulations for vaccination as a condition of deployment should be scrapped
Executive summary
For the avoidance of doubt, we strongly support vaccination against COVID-19, as there is clear evidence that it protects recipients from serious illness and death.
From the outset, we have argued that persuasion would likely be more successful than compulsion and that we need to balance the mitigated risk of infection with the risk of older and disabled people going without care. Our position remains the same.
We have written to the Secretary of State for Health and Social Care, the Rt Hon Sajid Javid MP, to call for the regulations requiring vaccination as a condition of deployment (VCOD) in CQC-regulated wider care settings to be withdrawn without delay. A copy of the letter is here
A clear distinction must be drawn, though, between the benefits of vaccination to the recipient and the alleged benefits of vaccination to others in contact with the recipient. The latter is the government’s justification for the regulations requiring vaccination as a condition of deployment (VCOD). It is claimed that if careworkers are vaccinated against COVID-19, the people they support will be safer.
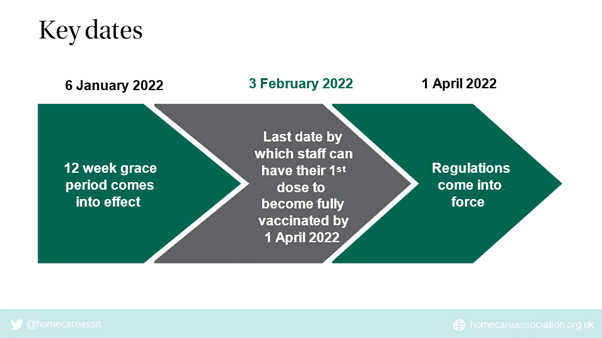
The regulations for extension of VCOD to the NHS and wider Care Quality Commission (CQC)-regulated settings, including homecare and extra care settings, were laid on 6 January 2022. The deadline for uptake of the first dose of vaccine is 3 February 2022 and for the second dose is 1 April 2022.
On 20 January 2022, only two weeks before the deadline for receipt of the first dose of vaccine, the government published its guidelines for implementation of vaccination as a condition of deployment for the delivery of CQC-regulated activities in wider adult social care settings.
The late publication of this guidance leaves little time for staff to make decisions about their future, now the scope has been clarified. Furthermore, if they have tested positive for COVID-19 recently, they may be in doubt about what this means for them if they are unable to be vaccinated before the deadline as planned. Guidance for obtaining temporary medical exemption after testing positive for COVID-19 has yet to be published, though is on its way. There may now be insufficient time for staff to be informed about how to apply for an exemption, to go through the process of applying for an exemption and, if they are refused, then to obtain a vaccine by the deadline.
These two pieces of guidance are vital for operational implementation of the regulations.
They explain that where a registered person employs or otherwise engages someone to provide a direct, face to face CQC-regulated social care activity, the registered person will need to obtain evidence that the individual:
- meets the vaccination requirements set out in the regulations;
- is medically exempt or;
- is covered by certain other exceptions.
Failure to obtain evidence of vaccination or exemption from a member of staff will result in dismissal of the member of staff on 1 April 2022. The employer may be subject to enforcement action by CQC if they do not implement the regulations correctly.
Standing back from the detail, what is the real risk to the safety of older and disabled people receiving homecare in wider settings of CQC-regulated care?
Even at the height of the first wave of the COVID-19 pandemic, without adequate PPE, testing or vaccines for homecare workers, death rates from COVID-19 in homecare were much lower than in care homes. Homecare is typically not delivered in a congregate setting and thus risk of transmission and infection is relatively low.
More recent ONS data show that deaths from COVID-19 in people’s own homes are far lower than from other causes, such as heart disease, dementias and some cancers. Thus, the inherent risk to older and disabled people from COVID-19 in homecare appears to be no different from that to people in the wider community.
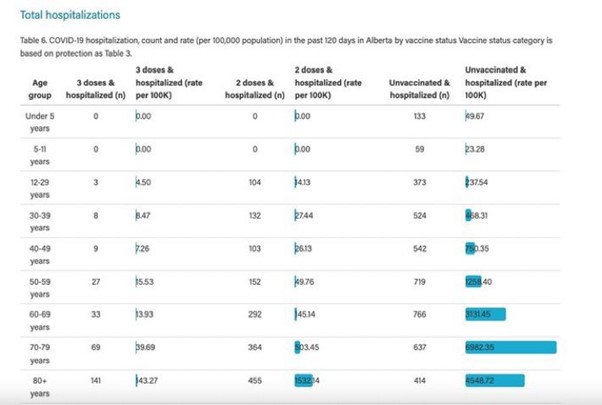
All older and disabled people have now been offered, and many have accepted, triple vaccination against COVID-19, which evidence clearly shows protects against serious illness and death. Data from Canada indicate that hospitalisation and death rates of triple-vaccinated people over 80 years old are lower than those of unvaccinated 12 to 29 year olds.
For over a year now, homecare workers have had access to ample supplies of free PPE, routine asymptomatic testing and vaccination, so multiple infection prevention and control measures are universally employed. Currently 81.8 per cent of homecare workers have been double-vaccinated.
The benefits of vaccination to the recipient can be clearly evidenced and every individual can make an informed decision about their own health based on current data.
Evidence to justify the stated benefits of the VCOD regulations is more questionable for the following reasons:
- Vaccination against COVID-19 does not appear to prevent transmission or infection, particularly with more recent variants, to a biologically relevant extent.
- A requirement for boosters is not included in the regulations, though immunity from vaccines obtained at least 12 months ago is known to provide insufficient protection against COVID-19. If boosters were included in the regulations, we would currently lose 64 per cent of the homecare workforce, as only 36 per cent of homecare workers had received a third dose of vaccine by 20 January 2022.
- COVID-19 transmission does not depend on a person’s employment status. An individual careworker that is self-employed and delivering personal care, as defined in the legislation, is exempt. In contrast, a careworker employed by a CQC-registered agency and delivering personal care is in scope.
- COVID-19 transmission does not depend on a person’s role title. A person employed or engaged by a CQC-registered agency to deliver an activity face-to-face, which is not on the list of regulated activities defined in the legislation, such as companionship or cleaning, is exempt. In contrast, a person with equivalent face-to-face contact with a client but delivering a regulated activity such as personal care is in scope.
At this late stage, it will be difficult for registered managers to deal with all the employment issues likely to arise, particularly as almost 20 per cent of homecare workers have yet to be vaccinated, according to data from Capacity Tracker on 20 January 2022. Within this, there is substantial regional variation, with some London boroughs recording vaccine uptake of homecare workers as low as 50 to 60 per cent.
The risks of losing 15 to 20 per cent of the homecare workforce, an estimated 75,000 to 100,000 homecare workers (based on Skills for Care and government data), at a time of already high levels of unmet need, are extreme.
An estimated 75,000 to 100,000 older and disabled people could be left without the care they need.
Already, informal and family carers are under intolerable pressure trying to support their loved ones without help.
Councils are unable to find available homecare and are having to ration care or place people in care homes when they would not have chosen that option.
NHS trusts are struggling to discharge people from hospital and have had to resort to offering financial inducements to families to take people home and setting up temporary “care hotels” for those who are supposedly medically fit for discharge. Inadequate capacity in community and social care is hampering the ability of the NHS to deal with both emergency demand and the elective backlog.
This lack of capacity is the result of years of central government under-investment in homecare at a time of rising population need, combined with labour market constraints arising from the UK's exit from the EU and the impact of COVID-19 on the care workforce.
In conclusion, we question why the government would choose to force dismissal from 1 April 2022 of up to one-fifth of the homecare workforce, up to 100,000 careworkers, when there is already severely inadequate capacity to meet demand. There is no evidence of high death rates from COVID-19 in people's own homes and the scientific basis for justifying the regulations is weak.
We have written to the Secretary of State for Health and Social Care, the Rt Hon Sajid Javid MP, to call on the government to:
- Recognise the high level of risk to older and disabled people of a further reduction in homecare capacity, as well as the difficulties this presents to councils and the NHS;
- Take note of official ONS data indicating that the risk of COVID-19 to people receiving homecare is relatively low and similar to that in the wider population, and that deaths from COVID-19 of people at home represent only 3 per cent of the total deaths of people at home.
- Acknowledge that the regulations as laid are based on questionable scientific evidence. For example, COVID-19 vaccines do not prevent or reduce transmission to a biologically relevant degree with all variants; double-vaccination 12 months ago is unlikely to protect the recipients or anyone else due to waned immunity; and it is plainly nonsense to suggest that transmission of COVID-19 is dependent on employment status or role title.
- Accept that the situation in wider society has changed from when the regulations requiring vaccination as a condition of deployment were first proposed and withdraw them without delay before employers have to start serving notice on employment contracts with vital homecare workers prior to 1 April 2022.
- Provide funding for targeted and tailored clinical support for careworkers with genuine fears and concerns about vaccination against COVID-19, so we can encourage more to accept vaccination to protect themselves.
- Invest adequately in homecare so we can build workforce capacity, address unmet need, reduce inequalities, extend healthy life expectancy of older and disabled people and reduce pressure on the NHS.
Homecare Association's Position
For the avoidance of doubt, we strongly support vaccination against COVID-19, as there is clear evidence that it protects recipients from serious illness and death.
Our position from the outset has not changed.
As soon as regulatory approval for the first vaccines was granted, we argued clearly in favour of vaccination against COVID-19 and expressed our belief that persuasion to achieve informed consent for uptake would likely be more successful than compulsion.
Importantly, we also advocated for careful consideration of balance of risk. Does the mitigated risk of infection from COVID-19 in triple-vaccinated older and disabled people at home really outweigh the risk of losing up to 20 per cent of the homecare workforce (c. 100,000 careworkers), resulting in c. 100,000 older and disabled people losing access to care? Who will care for them? What is the contingency plan? To this day, neither central nor local government have produced a credible response to these questions.
Risk of COVID-19 in homecare
Standing back from the detail, what is the real risk to the safety of older and disabled people receiving homecare in wider settings of CQC-regulated care?
For context, during the first wave of the COVID-19 pandemic in 2020, homecare workers had patchy access to appropriate PPE, no access to routine asymptomatic testing, and vaccines were not yet available. Despite this, deaths attributed to COVID-19 in homecare were much lower than in care homes,
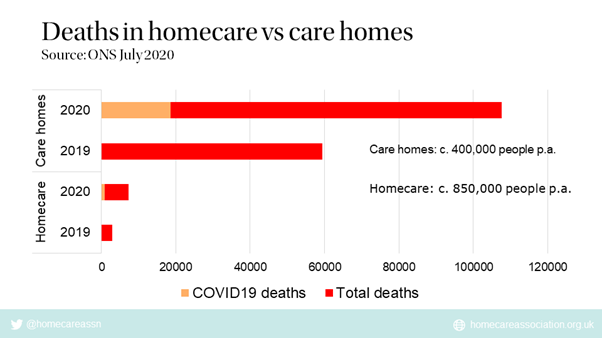
Unlike care homes, homecare is not delivered in a congregate setting. Average household size in the UK is 2.4 and larger households are relatively rare. Risk of transmission of COVID-19 is obviously much lower in a household of 1 to 3 people than in a care home with up to 120 residents sharing facilities.
Italian doctors at the epicentre of the first wave of COVID-19 suggested that the pandemic pointed to a need to shift from facilities-based to community-based models of care.
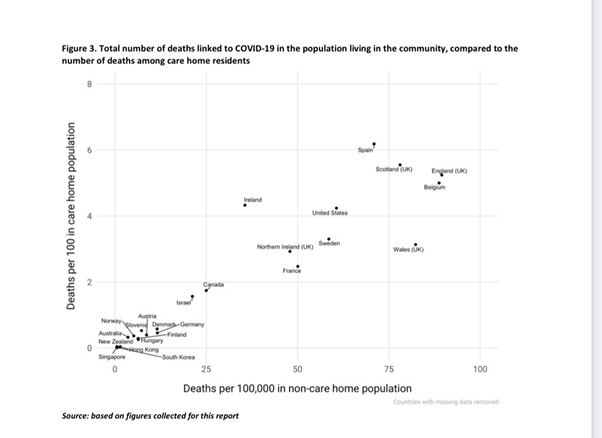
International evidence reveals a direct relationship between deaths from COVID-19 in the wider community and deaths from COVID-19 in care homes.
Among the homecare workforce, evidence suggests that the prevalence of COVID-19 is similar to that in the wider community.
Evidence indicates that the higher the spread of COVID-19 in the general population, the greater the risk to older and disabled people in care settings.
It is important to note that, whilst deaths from COVID-19 among people at home appear to be relatively low, excess deaths at home from causes such as heart disease, dementias and some cancers have increased substantially during the pandemic.
A combination of reasons may account for the increase in excess deaths at home, including
- Government advice in the first wave to stay at home to protect the NHS, which people generally obeyed, thus potentially not seeking necessary medical intervention;
- Fear of being a nuisance and adding pressure to healthcare services by seeking clinical help, thus not making appointments;
- Fear of infection reducing willingness to leave the home;
- Fear of being unable to visit loved ones in hospital, so more chose to die at home;
- Reduction in available outpatient clinics and increase in waiting lists, potentially affecting access to timely diagnosis and treatment;
- Undetected asymptomatic COVID-19 may have increased risk of death from certain conditions, such as heart disease.
As the pandemic progressed, by early 2021, good quality PPE, routine asymptomatic PCR testing and vaccination were readily available for homecare workers, further mitigating risk to those receiving care.
Vaccination against COVID-19 saves lives
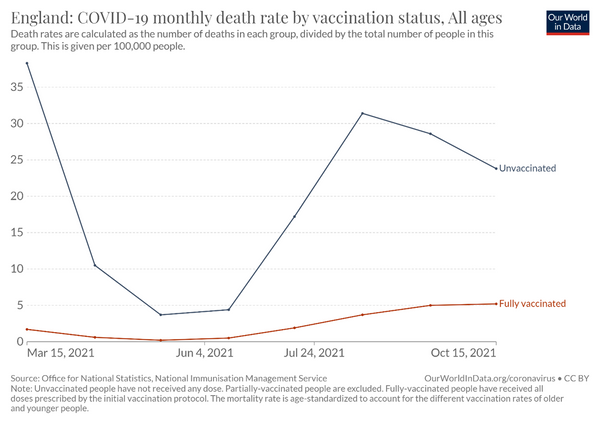
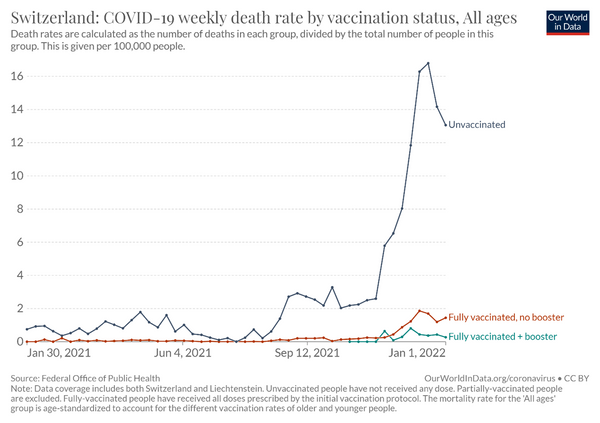
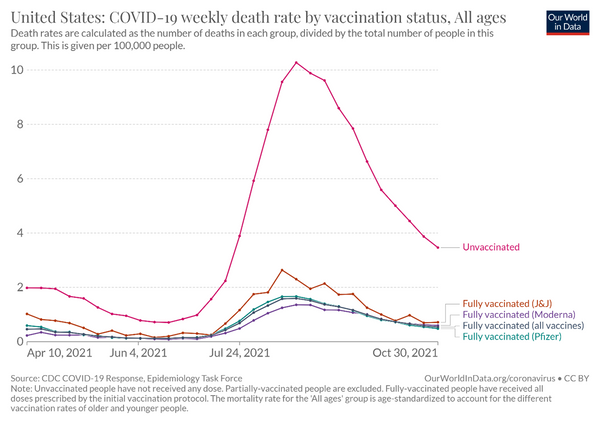
Little over a year after the first COVID-19 vaccine was administered in the UK, there is compelling international evidence that fully vaccinated people are at much lower risk of hospitalisation and death than unvaccinated people.
Recent data from Alberta, Canada, indicate that the hospitalisation rate among boosted 80+ year-olds is LOWER than the hospitalisation rate among unvaccinated 12-29 year-olds. If replicated elsewhere, this is powerful evidence for the protective effect of triple vaccination, even in higher risk groups. It also raises questions about the risks of removing infection prevention controls in wider society when many young people have not yet had the opportunity to be vaccinated, though risks of serious illness in younger people are typically relatively low.
The development and rollout of vaccines against COVID-19 is a remarkable scientific and operational achievement, which has clearly been of great benefit to many.
Despite this, there is a substantial proportion of the general population who have genuine fears and remain reluctant to accept the offer of vaccination against COVID-19; homecare workers are no exception.
Vaccine hesitancy in homecare
Common reasons given by homecare workers for their reluctance to be vaccinated are similar to those in the wider population, and include:
- Concerns about the apparent speed with which the vaccines were developed, leading some to question whether they have been adequately tested;
- Concerns that the vaccines are new and potential long-term side effects have not yet had time to manifest;
- Concerns based on internet misinformation, for example, about contents of the vaccines, fears about potential effects on fertility or lack of safety in pregnancy;
- General distrust of government for historic reasons, which is particularly prevalent in certain minority ethnic communities;
- Fear of needles;
- Cultural, religious or other beliefs;
- Belief that COVID-19 is a mild respiratory illness without serious risk, which is likely to be intensified if people have tested positive for COVID-19 without obvious symptoms.
Several months ago, we reached out to NHS England and local authorities for assistance with encouraging COVID-19 vaccine uptake among remaining homecare workers with genuine fears. Our aim was to ensure availability of tailored small group and one-to-one conversations with clinicians from similar communities to the care workers. Colleagues have been extremely supportive but the reality on the ground is that most of the attention and resource continues to be directed to care homes.
We remain fully committed to continuing work with colleagues in NHS England, DHSC and local government to seek to persuade homecare workers to accept vaccination against COVID-19 for their own health and safety.
Regulations for vaccination as a condition of deployment
Following widespread criticism for not doing enough to protect the health of older and disabled people in care homes in the first wave of COVID-19, the UK government decided to make vaccination a condition of deployment in care homes from 11 November 2021.
Care home workers that were not fully vaccinated by 11 November 2021 had to leave or be dismissed from employment. By 9 November 2021, over 45,000 care home workers had not been double vaccinated and thousands of others had already left prior to this point.
Whilst VCOD was being implemented in care homes, the government issued a consultation on extending vaccination as a condition of deployment (VCOD) to the NHS and wider CQC-regulated care settings, including homecare.
The justification given for requiring vaccination as a condition of deployment is that vaccination allegedly protects others in contact with the recipient, by reducing transmission and infection.
Though a majority of respondents did not support extension of the proposed regulations on vaccination as a condition of deployment, the government decided to press ahead regardless, ignoring warnings about risks of losing vital health and careworkers at a time of rising demand, as well as emerging evidence that vaccinated people can still transmit COVID-19.
The regulations for extension of VCOD to the NHS and wider CQC-regulated settings were laid on 6 January 2022. The deadline for uptake of the first dose of vaccine is 3 February 2022 and for the second dose is 1 April 2022.
Booster doses are currently not included in the regulations, despite evidence of waning immunity from the first two doses and the importance of booster vaccines in “topping up” protection. The government says it will keep the scope of the regulations under review.
If boosters were included in the regulations, we would currently lose 64 per cent of the homecare workforce, as only 36 per cent of homecare workers had received a third dose of vaccine by 20 January 2022.
On 20 January 2022, only two weeks before the deadline for receipt of the first dose of vaccine, the government published its guidelines for implementation of vaccination as a condition of deployment for the delivery of CQC-regulated activities in wider adult social care settings.
The guidance is important because it makes clear what is in and out of scope of the regulations. It will thus play a vital role in helping managers to discuss the policy with staff members who are unsure where they stand and are yet to make decisions; for example, those who think they may be eligible for an exemption. It may not give sufficient time for staff to be informed about how to apply for an exemption, to go through the process of applying for an exemption and, if they are refused, then to obtain a vaccine by the deadline.
The regulations mean that where a registered person employs or otherwise engages someone to provide direct, face to face CQC-regulated social care activity, the registered person will need to obtain evidence that the individual:
● meets the vaccination requirements set out in the regulations;
● is medically exempt or;
● is covered by certain other exceptions.
Failure to obtain evidence of vaccination or exemption from a member of staff will result in dismissal of the member of staff on 1 April 2022.
Vaccination and transmission of COVID-19
To reiterate, we strongly support vaccination against COVID-19 because there is clear evidence, as highlighted above, that vaccines protect the recipient from serious illness and death.
It is less clear, however, that vaccines against COVID-19 protect others in contact with the recipient by reducing transmission or infection to a biologically relevant extent, as claimed.
Papers in the scientific literature suggest that transmission of both the Delta variant and the Omicron variant of COVID-19 is higher in unvaccinated than vaccinated people, but vaccinated people can still spread COVID-19.
In the UK, 70.4 per cent of the population are fully vaccinated against COVID-19.
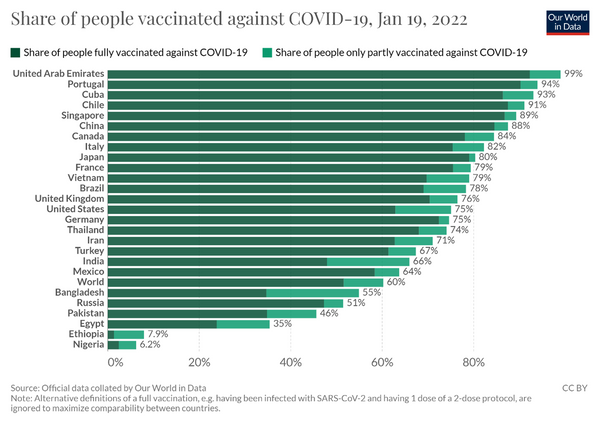
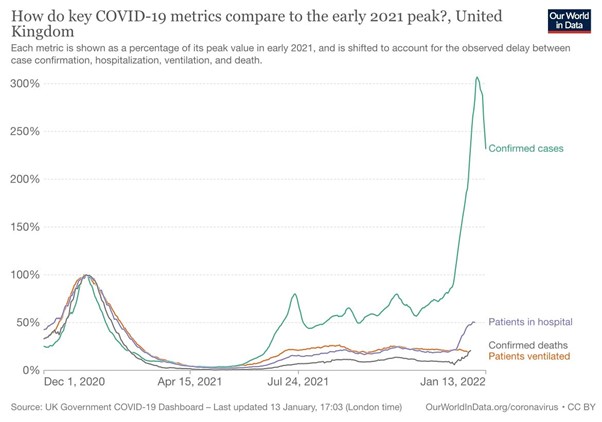
Despite generally high vaccination uptake, the Omicron variant of COVID-19 still spread like wildfire in the UK population.
In care homes, vaccination rates of both residents and staff are over 90 per cent but 60 per cent of care homes are currently reporting outbreaks.
The benefits of vaccination to the recipient are, however, evident in the relatively low proportion of hospitalisations and deaths from COVID-19 in the UK.
Vaccines that stop transmission are often against viruses that replicate internally first and only then transmit, such as measles. So, if the vaccine stops internal replication, it stops transmission.
COVID-19, however, is able to land in the nose, replicate within the first available mucus tissue it encounters with ACE-expressing cells and transmit on, without requiring systemic infection.
It thus appears that one of the main justifications for the VCOD regulations – that vaccination protects others in contact with a recipient by substantially reducing or preventing transmission and infection – is over-stated.
Exemptions from VCOD regulations
Bizarrely, the government has decided to apply the VCOD regulations only to staff employed or otherwise engaged by CQC-registered agencies, delivering regulated activities, such as personal care or treatment of disease, disorder or injury, face-to-face.
Careworkers who deliver personal care face-to-face but do not work for a CQC registered agency, for example personal assistants, are exempt. There are at least 130,000 careworkers that fall into this category.
Furthermore, staff who deliver unregulated activities, such as companionship or cleaning, despite face-to-face contact with clients, are also exempt.
This suggests that Ministers, or their scientific advisors, believe that transmission of COVID-19 is dependent on a person’s employment status and job title, which is plainly nonsense.
Reasons why the VCOD regulations are ridiculous
A clear distinction must be drawn between the benefits of vaccination to the recipient and the alleged benefits of vaccination to others in contact with the recipient. The latter is the government’s justification for the VCOD regulations – they claim that if careworkers are vaccinated against COVID-19, the people they support will be safer.
The benefits of vaccination to the recipient can be clearly evidenced and every individual can make an informed decision about their own health based on current data.
Evidence to justify the stated benefits of vaccination to others in contact with the recipient is more questionable for the following reasons:
- Vaccination against COVID-19 does not appear to prevent transmission or infection to a biologically relevant extent, particularly with more recent variants.
- A requirement for boosters is not included in the regulations, though immunity from vaccines obtained at least 12 months ago is known to provide insufficient protection against COVID-19. If boosters were included in the regulations, we would currently lose 64 per cent of the homecare workforce, as only 36 per cent of homecare workers had received a third dose of vaccine by 20 January 2022.
- COVID-19 transmission does not depend on a person’s employment status. An individual careworker that is self-employed and delivering personal care, as defined in the legislation, is exempt. In contrast, a careworker employed by a CQC-registered agency and delivering personal care is in scope. This makes little sense.
- COVID-19 transmission does not depend on a person’s role title. A person employed or engaged by a CQC-registered agency to deliver an activity face-to-face, which is not on the list of regulated activities defined in the legislation, such as companionship or cleaning, is exempt. In contrast, a person with equivalent face-to-face contact with a client but delivering a regulated activity such as personal care is in scope. This also makes little sense.
On top of this, the government has left only two weeks between publication of the operational guidelines for VCOD and the deadline for the first dose, which makes this policy extremely difficult to deliver in practice, particularly as so many careworkers have yet to be vaccinated.
The late publication of this guidance leaves little time for staff to make decisions about their future. Furthermore, if they have tested positive for COVID-19 recently, they may be in doubt about what this means for them. Guidance for obtaining temporary medical exemption as a result of testing positive for COVID-19 has yet to be published, though is on its way.
Uptake of COVID-19 vaccines in homecare
As the situation stood on 20 January 2022, unpublished data on uptake of vaccines in homecare from Capacity Tracker were as follows:
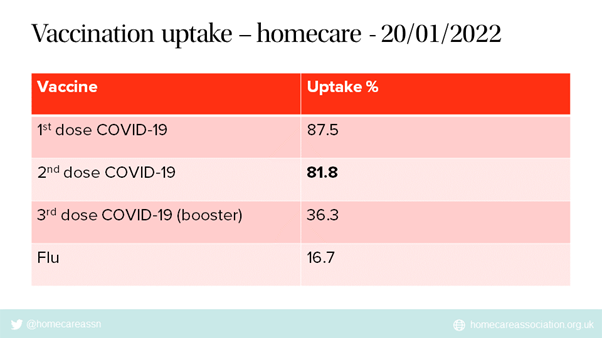
This means that unless there is a substantial surge in uptake of vaccination in the next two weeks, which appears unlikely, we are set to lose nearly 20 per cent of the homecare workforce, which according to Skills for Care data equates to c. 100,000 homecare workers.
As there is approximately one careworker for every person receiving homecare across the sector, this could result in c. 100,000 older and disabled people losing access to care.
Risks of VCOD regulations
The Association of Directors of Adult Social Service (ADASS) reported in November 2021 and January 2022 that unmet need is high and councils are struggling to source homecare, despite record growth in provision. Due to additional pressures caused by the spread of COVID-19, all directors are, unwillingly, having to implement contingency actions they find unacceptable. Actions include prioritising life sustaining care such as supporting someone to eat and remain hydrated over supporting someone to get out of bed or complete other activities; being unable to undertake reviews of risk at all or to rely for this on the views of providers, family carers or people using services themselves; and leaving people with dementia, learning disabilities or poor mental health isolated or alone for longer periods than usual.
Inadequate homecare capacity is also reportedly leading to an increase in numbers of patients stranded in NHS hospitals. Others are being placed in care homes or so-called “Care Hotels” when they would rather go home. In some areas, NHS trusts have offered payments to family members to take their relatives home from hospital.
Inability to discharge people from hospital in a timely manner is contributing to ambulance queues and making it harder for NHS colleagues to reduce waiting lists. Some clinicians have said that patient care is being severely compromised as a result.
Homecare Association members report that recruitment and retention of careworkers is more difficult than anyone can remember. In November 2021, 85% of respondents in a survey of homecare providers (n=339) said that recruitment is the hardest it has ever been. At the same time, careworkers are leaving in droves for better paid jobs in retail and hospitality where vaccination is not required.
Regulations enforcing vaccination as a condition of deployment will further exacerbate this situation.
Why would we choose to dismiss up to one-fifth of the homecare workforce, when there is already severely inadequate capacity to meet demand? There is no evidence of high death rates from COVID-19 in people’s own homes and the scientific basis for justifying the regulations is weak.
As we have argued all along, though we believe strongly in the benefits of vaccination per se, we consider that the risks of implementing the VCOD regulations far outweigh any potential benefits. The regulations should never have been introduced and now should be withdrawn.
Adding further weight to this contention is the fact that, on 19 January 2022, the Secretary of State for Health and Social Care, the Rt Hon Sajid Javid MP announced an end to “Plan B” COVID-19 restrictions. People will no longer be advised to work from home, face coverings will no longer be mandatory in indoor venues, and organisations will be able to choose whether to require NHS COVID Passes. The government has also talked about the possibility of bringing forward the end of self-isolation regulations, so those who are infected with COVID-19 are free to interact with others. They may also cease to provide free LFD test kits to the general public.
As the government appears to have decided that the pandemic is coming to an end, and favours a libertarian approach to infection prevention and control, it seems inconsistent for Ministers to start implementing complex new COVID-19 regulations.
Conclusion
To reiterate, we strongly support vaccination against COVID-19, as there is clear evidence that it protects recipients from serious illness and death.
A clear distinction must be drawn between the benefits of vaccination to the recipient and the alleged benefits of vaccination to others in contact with the recipient. The latter is the government’s justification for the VCOD regulations. It is claimed that if careworkers are vaccinated against COVID-19, the people they support are safer.
Death rates from COVID-19 among people receiving homecare are relatively low compared with care homes, as homecare is typically not delivered in congregate settings where risk of transmission is intrinsically higher. Death rates from COVID-19 among people at home, including those receiving homecare, are low, only 3% of total deaths, with the remaining 97% attributed to other causes including heart disease, dementia and some cancers. The inherent risk to older and disabled people from COVID-19 in homecare appears to be no different from that to people in the wider community.
All older and disabled people have now been offered, and many have accepted, triple vaccination against COVID-19, which evidence clearly shows protects against serious illness and death.
Homecare workers have access to ample supplies of free PPE, routine asymptomatic testing and vaccination, so multiple infection prevention and control measures are universally employed. Currently 81.8% of homecare workers have been double-vaccinated.
Evidence to justify the stated benefits of the VCOD regulations is questionable for the following reasons:
- Vaccination against COVID-19 does not appear to prevent transmission or infection to a biologically relevant extent, particularly with more recent variants.
- A requirement for boosters is not included in the regulations, though immunity from vaccines obtained at least 12 months ago is known to provide insufficient or even zero protection against COVID-19. If boosters were included in the regulations, we would currently lose 64 per cent of the homecare workforce, as only 36 per cent of homecare workers had received a third dose of vaccine by 20 January 2022.
- COVID-19 transmission does not depend on a person’s employment status.
- COVID-19 transmission does not depend on a person’s role title.
On top of this, the government has left only two weeks between publication of the operational guidelines for VCOD and the deadline for the first dose, which makes this policy extremely difficult to deliver in practice, particularly as so many careworkers have yet to be vaccinated.
The risks of losing up to 20 per cent of the homecare workforce, an estimated 100,000 careworkers, at a time of already high levels of unmet need, are extreme.
In conclusion, we question why the government would choose to force dismissal from 1 April 2022 of up to one-fifth of the homecare workforce, up to 100,000 careworkers, when there is already severely inadequate capacity to meet demand. There is no evidence of high death rates from COVID-19 in people's own homes and the scientific basis for justifying the regulations is weak.
We have written to the Secretary of State for Health and Social Care, the Rt Hon Sajid Javid MP, to call on the government to:
- Recognise the high level of risk to older and disabled people of a further reduction in homecare capacity, as well as the difficulties this presents to councils and the NHS;
- Take note of official ONS data indicating that the risk of COVID-19 to people receiving homecare is relatively low and similar to that in the wider population, and that deaths from COVID-19 of people at home represent only 3 per cent of the total deaths of people at home.
- Acknowledge that the regulations as laid are based on questionable scientific evidence. For example, COVID-19 vaccines do not prevent or reduce transmission to a biologically relevant degree with all variants; double-vaccination 12 months ago is unlikely to protect the recipients or anyone else due to waned immunity; and it is plainly nonsense to suggest that transmission of COVID-19 is dependent on employment status or role title.
- Accept that the situation in wider society has changed from when the regulations requiring vaccination as a condition of deployment were first proposed and withdraw them without delay before employers have to start serving notice on employment contracts with vital homecare workers prior to 1 April 2022.
- Provide funding for targeted and tailored clinical support for careworkers with genuine fears and concerns about vaccination against COVID-19, so we can encourage more to accept vaccination to protect themselves.
- Invest adequately in homecare so we can build workforce capacity, address unmet need, reduce inequalities, extend healthy life expectancy of older and disabled people and reduce pressure on the NHS.