Homecare – the need to change public opinion
On 13 May 2022, I represented the voice of homecare providers at a round table with the Secretary of State for Health and Social Care, Rt Hon Sajid Javid MP. The event was attended by care representative organisations, major charities and a representative of people who draw on care and support services.
The Secretary of State wanted to hear our views on the progress of the social care reform agenda and to listen to any other issues on our minds. Each participant was given the opportunity to speak and highlight matters of importance to those they represent. In truth, in the time available we were able only to scratch the surface of the issues at hand.

All participants welcomed the vision articulated in the two White Papers on Adult Social Care Reform and Integration, though reflected that the gap between reality and ambition appears to be widening and funding to implement the reforms is inadequate.
Unmet need and workforce
With a new report from the Association of Directors of Adult Social Services (ADASS) highlighting an increase in unmet need, and Skills for Care data showing vacancy rates among the highest on record, workforce was a hot topic.
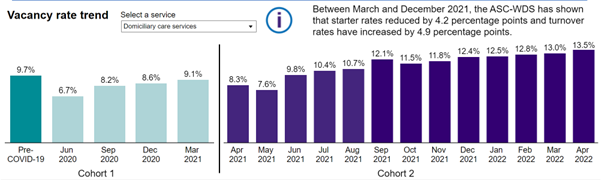
Source: Skills for Care, April 2022
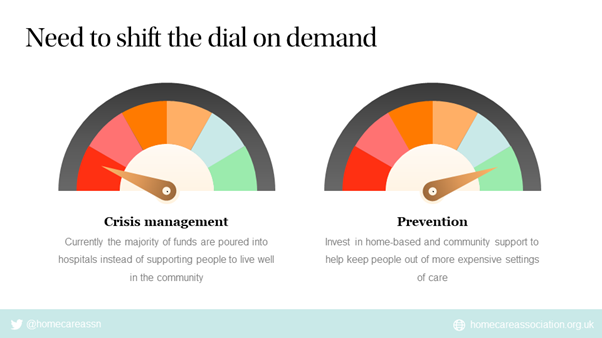
Right now, there are insufficient care workers to support people to live well in their communities and demographic pressures are continuing to increase. Failure to adopt a strategic approach to workforce planning or to shifting the demand curve, preventing ill-health and meeting need, risks unsustainable strain on health and care services.
On top of this, the impact of COVID-19 on longer-term population health appears not to have been factored in and, in any case, the UK government has rejected responsibility for modelling future workforce needs.
Low numbers of care workers relative to the population aged 65+ persist in most OECD countries.
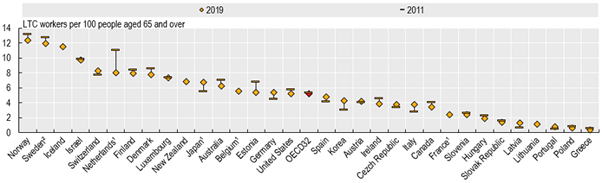
Source: OECD Health Statistics 2021, complemented with EU-LFS.
We spoke about the skilled professionals working in social care, the need to value them and to create rewarding careers. Over the next three years, the government has allocated £500m for workforce development which will help. This will not, however, be enough to improve pay, terms and conditions of employment. Without adequate pay and salary differentials between levels, it is hard to professionalise the workforce and create meaningful career pathways.
Many countries are experiencing a shortage of skilled care workers and are competing for workers willing to migrate. Cost and complexity of immigration to the UK limits numbers. Given the generally low fee rates for state-funded homecare, it is difficult for employers to meet the salary threshold for a Health and Care Visa. Delivering homecare in many places requires driving a car, which is an additional barrier for overseas workers, as is lone working.
Doubling the number of careworkers to cope with a doubling of demand over the next 30 years is unlikely to be a realistic proposition and we need to consider other solutions.
Collaboration and innovation
When I spoke, I reflected on the opportunities for new ways of multi-disciplinary working within Integrated Care Systems, and the use of technology solutions and big data, to support us all to live well at home and extend healthy life expectancy.
Currently it is difficult to realise the ambitions of the care and health reform agenda and the potential of new ways of working and technology solutions.
Commissioning and purchase of homecare needs overhauling
There is currently inadequate investment to enable new models of commissioning, purchase and delivery of home-based support and care, focused on improving outcomes and growing and developing the workforce.
Time and task purchase of homecare mitigates against retention and recruitment of careworkers. It is also a barrier to the use of technology solutions focused on improving outcomes, as payment is for process not results. Inadequate fee rates for state-funded services mean that margins are tight and there is little cash to invest in either systems or people.
Different approaches to commissioning and purchase of homecare, which enable more autonomy for both people drawing on services and providers, flexibility to adjust services to changing need, and security of income, whilst also covering costs, would be highly beneficial.
New models
Ways of working across health and care systems need a radical re-think. In most places, GPs are set up to be the gatekeepers of almost everything and they cannot cope. Homecare providers that have tried to generate and use data in a predictive and preventative way have been told by some GPs that they don’t have the time to help. And frequently they don’t.
We need new ways of working which enable collection, analysis and use of multiple sources of data in a predictive way and agile approaches to acting on the data. For example, if motion sensors indicate that a person at home has fallen but there is nobody to go and pick them up, how does it help? If a person’s blood pressure is monitored in real-time and a deviation from normal is detected, but GPs have no time to see them, how does it help?
New types of data-driven, responsive services need to be configured to support people at home in an efficient and effective way, which includes people paying for their own care as well as those funded by councils or the NHS.
Culture
Other health and care professionals appear to look down on homecare workers, who are often ignored and left to fight the corner of the people they support on their own.
Homecare workers spend more time with people drawing on services than any other professional and understand their needs better. This fact could be used positively, especially as councils are unable to keep pace with assessments needed, with over half a million people currently waiting.
Right now, we are losing homecare workers at a faster rate than ever, which is contributing to unmet need in the community and major issues for NHS trusts with discharging people from hospital when ready to go home.
In turn, this is contributing to greater burdens on the NHS – there are more people with deteriorating health; longer ambulance response times; cancelled clinics; cancelled operations; and difficulty in reducing waiting lists.
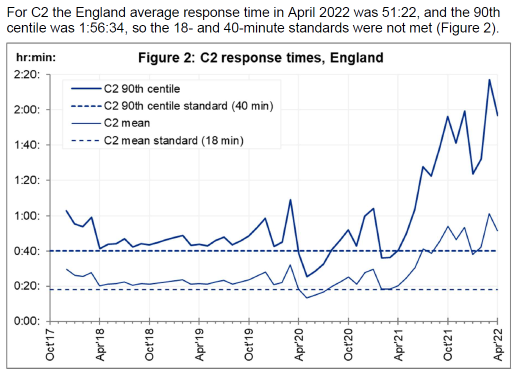
Ambulance response times (C2 - emergencies), NHS England, May 2022
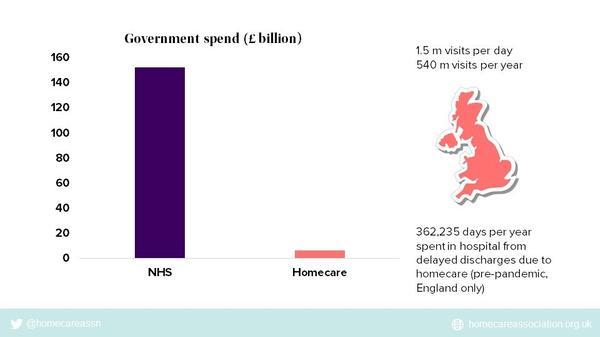
Need to invest in homecare
Under-investment in homecare relative to the NHS makes little sense, especially because this has led to poor pay, terms and conditions of employment and an unstable and insufficient workforce.
Homecare workers have been further disadvantaged by removal of the Infection Control and Testing Fund from 1 April 2022, which previously enabled employers to pay staff full wages whilst isolating after a positive COVID-19 test result. Unlike wider society, isolation after a positive test is still required for health and care workers. Now most homecare workers receive no pay for the first 3 days and then just Statutory Sick Pay (SSP) of £99.35 per week from day 4. SSP is at least 2 to 3-fold lower than typical careworker wages. Careworkers are leaving for jobs where either isolation is not required, or income is not affected by sickness absence.
On top of this, high fuel costs are also hitting the pockets of homecare workers and they are leaving for jobs without the need for travel.
Despite the recognised importance of high quality and sustainable homecare in Integrated Care Systems, the government is progressively weakening services by pouring most of the available funding from the Health and Social Care Levy into the NHS and starving social care.
Funding Reform and Fair Cost of Care
Regrettably, the adult social care funding reforms risk making the situation worse. The concept of a Fair Cost of Care is a good one – the idea that public sector commissioners should pay rates for care that cover costs. Indeed, we believe it should be unlawful for public sector organisations to purchase care at rates below the costs of compliance with employment and care regulations, and of running sustainable services.
Implementing the Fair Cost of Care reform with ten times too little funding, however, risks major destabilisation of services.
Widening the scope of s.18 (3) of the Care Act 2014, which enables councils to purchase care for self-funders at the fee rates local authorities pay, could be catastrophic if local authority fee rates do not increase sufficiently. Providers risk losing vital additional income from self-funders and becoming insolvent.
In homecare, s.18 (3) of the Care Act 2014 has been in force since 2015. Up to now, it has mostly been applied to people discharged from hospital on NHS funding and then requiring ongoing support. In future, more people are likely to become aware of the existence of this legislation, as assessments will be needed to start the care cap clock ticking.
Currently, councils cannot keep pace with assessments for people needing state-funded services, so there is little chance of them being able to cope with assessing self-funders too.
When self-funders are kept waiting for assessment, or realise that their needs are deemed not to be eligible for funding, or that they do not meet the financial threshold for funding, their dissatisfaction will grow and councils will likely receive many appeals, causing further delays.
Caring as an electoral issue
Governments respond to what they perceive to be public opinion.
Recent polling by Opinium for Progressive Britain, suggests that social care is fairly low down the list of topics that people feel passionate about.
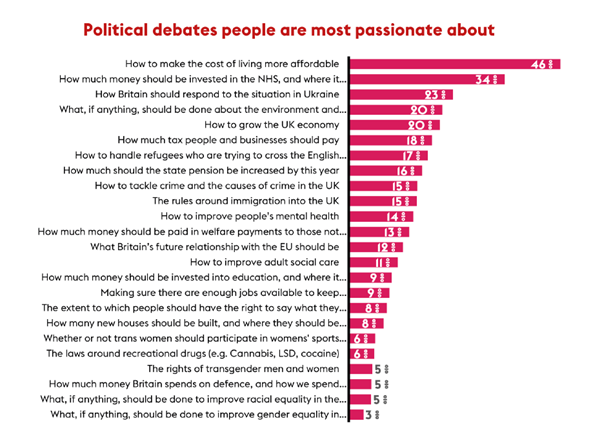
HM Treasury is clear that no more money will be made available for social care in this Spending Review period. Most of what is raised is going to the NHS. As the polling data show, voters are highly interested in how much money should be invested in the NHS and pay much less attention to social care.
If we are to change this situation, we need to raise public awareness of the value of homecare and ensure that people understand that the NHS cannot function effectively without investment in homecare and other community services.
If you have ideas about how, collectively, we can continue to raise the profile of homecare and shift public opinion, please join the debate and send us your thoughts by email at: [email protected]
Dr Jane Townson
CEO, Homecare Association





